Could we say ….
that even one death resulting from a suicide is acceptable in mental illness? Clearly, we wouldn’t want that one person to be OUR relative, neighbor, friend, right? That one person can’t be anyone’s relative, neighbor or friend. So zero deaths by suicide should be our goal.
Are you a clinician dissatisfied with the suicide prevention approach used at your center? Or perhaps are you a survivor concerned that suicidal feeling will recur and you question who or what is going to truly help you??? Or maybe you’re someone whose relative attempted suicide last year and was found in time, and you’re hunting for a more proactive and effective suicide prevention program but unsure where to turn?
I have an approach that I’d like you to consider for your clients, or for yourself or for your loved ones: I recommend the Zero Suicide (www.zerosuicide.com) program. Zero Suicide, an approach and program developed for the health care system, views suicide deaths as a preventable outcome and insists that the goal of zero suicides among persons receiving care is a goal that system can and should accept!
Zero Suicide, a project of the Suicide Prevention Resource Center (SPRC), grew from work done by the National Action Alliance on Suicide Prevention (NAASP). It is a specific set of tools and strategies. It is a concept, a practice, and a goal.
NAASP views suicide as preventable and the goal of zero suicides as a goal we should all aspire to accomplish. The word ALL is significant. This initiative requires the engagement of suicide attempt survivors, family members, policymakers, and researchers, and the clinic or hospital. The effort seen by the NAASP and Zero Suicide is a community endeavor—an effort including but beyond health care providers and clinicians. Beyond heroic efforts of individual practitioners.
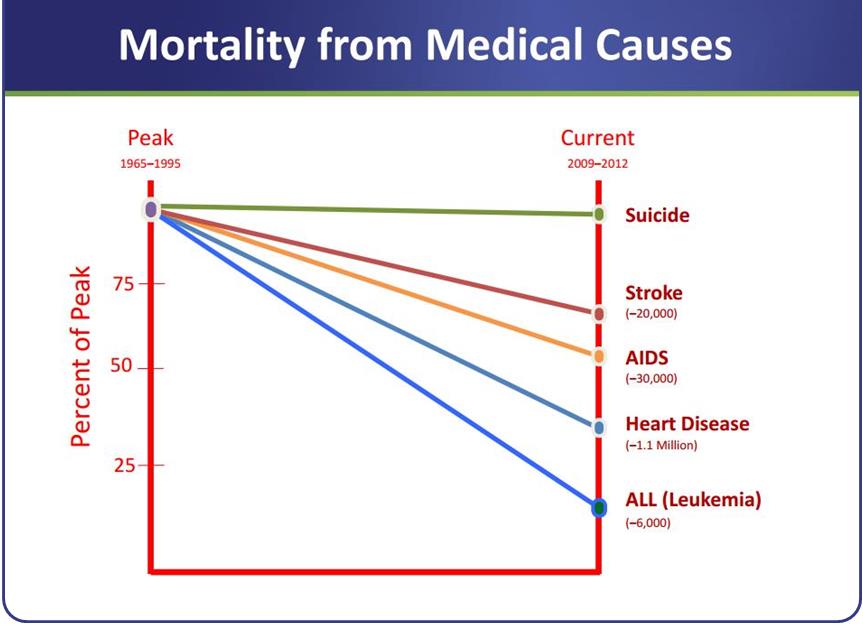
Where did this Zero Suicide program come from? The approach builds on work done in several health care organizations, including the Henry Ford Health System (HFHS) in Michigan. The Henry Ford Health System had already applied a rigorous quality improvement process to problems such as inpatient falls and medication errors. They also realized that mental and behavioral health care could be similarly improved … an individual involved with the quality improvement group challenged the team: “Why don’t we adopt zero suicide as our improvement goal?” As a result HFHS developed the Perfect Depression Care model, a comprehensive approach that included suicide prevention as an explicit goal. Both best and promising practices in quality improvement and evidence-based care are applied in their model and they have had wonderful, life-affirming results—-an 80% reduction in the suicide rate among health plan members.
NAASP’s Clinical Care and Intervention Task Force then identified essential elements of suicide prevention for health care systems having a defined population of individuals with mental illness. The Zero Suicide approach is created around these essential elements.
Here’s what I like about their approach:
Zero Suicide asks for a change in culture with firm leadership buy-in. The workforce – this includes both clinical and non-clinical staff – is to be trained using the Zero Suicide Toolkit. The cultural milieu is to foster a caring, non-judgmental workforce. Considerate and compassionate caring has sometimes been absent when the person being cared for has attempted or considered suicide (c.f. The Way Forward report). Suicide risk among people receiving care is identified and assessed systematically. Every person has a suicide care management plan, or pathway to care, that is timely and adequate to meet their needs. Finally, I’m very encouraged that this planning includes collaborative safety planning and restriction of lethal means.
It is also vital that treatment address the person’s suicidality. The patient’s own suicide planning needs to be discussed in detail and taken apart and turned into a scenario where the person is once again safe. Contact and support for the suicidal person, especially when in transition between emergency room and home or inpatient care and home, must be continuous. Many suicides occur after discharge from the hospital or emergency room (c.f. The Way Forward and Continuity of Care for Suicide Prevention reports). Deaths that occur after discharge aren’t inevitable; they can be tackled by better transition and discharge planning with greater attention to detail.
Fellow advocates, we can do better. Zero Suicide’s program can help.