Good day! I officially launched my website and blog last Friday and Saturday at the NAMI (National Alliance on Mental Illness) Wisconsin Conference. So many friends and colleagues expressed interest and well wishes to me that I am more eager to write than ever.
I took yesterday off to spend an afternoon hiking the prairie and woodsy grounds of one of my favorite places, the International Crane Foundation (ICF) near Baraboo, WI. It was so serene and peaceful that I was able to see long and deep. Today I find my mind is free and my body is relaxed to think and write.
I will focus on prevention of suicide in my coming posts this spring. Particularly on advances in suicide prevention. Why? I believe suicide prevention should be a top priority for mental health organizations and concerned individuals, indefinitely. The US suicide rate is unchanged in 2 decades. Mortality from various medical causes has decreased (see charts below).
In hope of gathering current material on advances in suicide prevention, I am traveling to Stevens Point on Wednesday to attend another conference. The conference theme is “Communities in Action to Prevent Suicide” put on by Prevent Suicide, Wisconsin and sponsored by Mental Health America (MHA). There are two nationally known keynote speakers from the prevent suicide movement featured. I am eager to hear what they have to say and the advice they have to give.
I will couple the information from the Stevens Point conference with the conclusions and recommendations offered in the report The Way Forward: Pathways to hope, recovery, and wellness with insights from lived experience, National Action Alliance for Suicide Prevention: Suicide Attempt Survivors Task Force. (2014). The report is available on my Resources On Suicide page. My hope is that you will feel better informed to look at suicide prevention practices in your area and seek input, if needed, and to update local policies and procedures to save more lives.

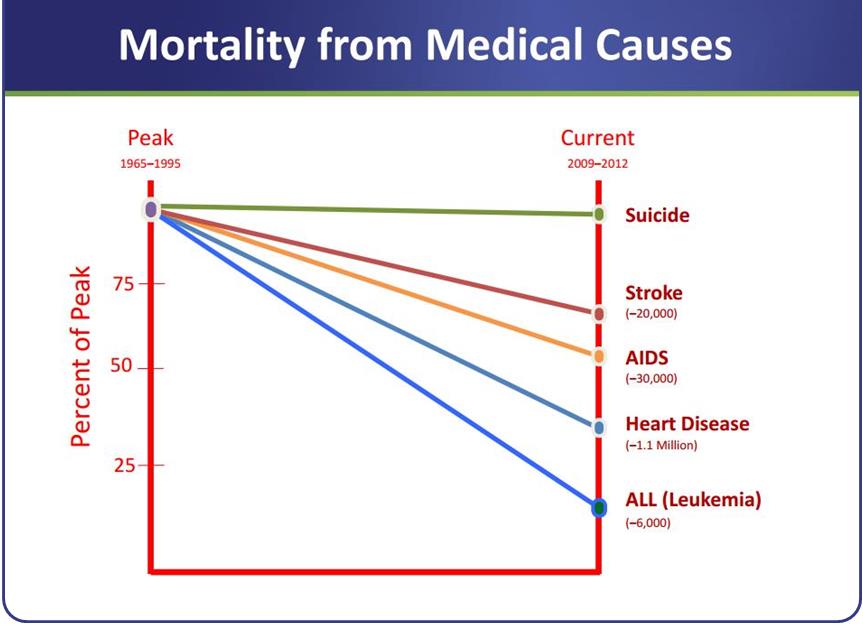
These graphs from a keynote presentation by Dr. Thomas Insel, Director of National Institute of Mental Health at the NAMI annual convention
